
Most parents know the panic of a sudden ear ache in the middle of the night. By age three, over 80 percent of children experience at least one middle ear infection. It is frustrating, painful, and often confusing to decide whether your child needs medication or just time to heal.
Otitis Media is a medically defined inflammation or infection of the air-filled space behind the eardrum. Also known as middle ear infection, it ranks among the most frequent reasons for doctor visits in pediatrics. While often associated with colds, the underlying mechanics involve fluid trapping that creates a breeding ground for bacteria.
How Fluid Traps Behind the Eardrum
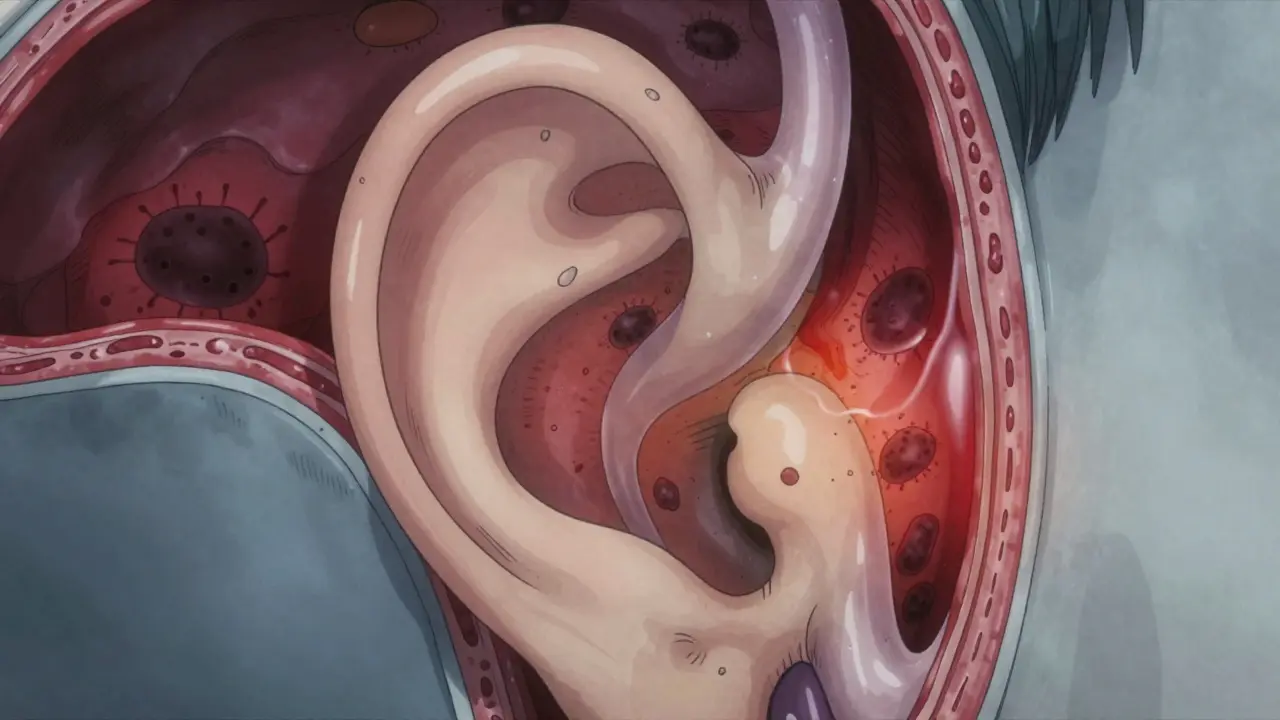
To understand why these infections happen, you have to look at the anatomy. Your middle ear connects to the back of your throat via a small channel called the Eustachian Tube. In healthy adults, this tube opens regularly to equalize pressure and drain mucus. However, in young children, this tube sits at a much more horizontal angle. This immature structure functions less efficiently than the vertical tubes found in adults.
When a child catches a cold, the lining of this tube swells. If the swelling blocks the passage, fluid becomes trapped in the middle ear space. This environment is warm and stagnant, allowing pathogens to multiply rapidly. Research from Yale Medicine notes that household cigarette smoke increases this risk by 50 percent because smoke irritates the lining of these delicate tubes. Without proper drainage, pressure builds up until the eardrum bulges outward, causing the sharp pain children often describe.
Distinguishing Between Acute Infection and Fluid Buildup
Not every fluid buildup requires immediate antibiotics. Doctors distinguish between two main conditions. Acute Otitis Media (AOM) represents the sudden-onset infectious form characterized by middle ear swelling, fluid accumulation, pain, and often fever. On the other hand, Otitis Media with Effusion (OME) describes the persistent fluid buildup that follows the resolution of the acute infection. In OME cases, there is no active infection, so antibiotics provide little benefit. Understanding this difference prevents unnecessary drug use.
The Role of Germs in Ear Infections
Identifying the cause helps determine the right treatment. Most ear infections stem from bacterial agents like Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. These bacteria thrive when the immune system is distracted by viruses such as the flu or RSV. While many mild infections resolve on their own, severe cases require targeted intervention. Data from the Centers for Disease Control shows that 30 to 50 percent of pneumococcal isolates demonstrate some penicillin resistance. This resistance pattern drives the decision to use high-dose dosing rather than standard doses.
Antibiotic Guidelines and Watchful Waiting
Deciding whether to prescribe medication involves balancing benefits against risks. The American Academy of Pediatrics (AAP) recommends a nuanced approach. For children under six months with definite AOM, antibiotics are always necessary due to developing immune systems. However, for older children aged two years and up with mild symptoms, observation without drugs is often safe. This "watchful waiting" strategy relies on the fact that 80 percent of uncomplicated AOM cases resolve spontaneously within three days.
| Age Group | Symptom Severity | Standard Action |
|---|---|---|
| Under 6 Months | Mild to Severe | Treat Immediately |
| 6 Months to 23 Months | Mild | Observation Allowed |
| 6 Months to 23 Months | Severe | Treat Immediately |
| 24 Months or Older | Mild to Moderate | Observation Allowed |
| 24 Months or Older | Severe | Treat Immediately |
First-Line Medications and Dosage Logic
If antibiotics become necessary, Amoxicillin remains the gold standard. Current clinical guidelines suggest a dose of 80 to 90 mg/kg/day for children under two years with bilateral infections. This high dose ensures the medicine reaches concentrations strong enough to kill resistant bacteria. For those allergic to penicillin, alternatives include ceftriaxone given as an injection, cefdinir taken orally, or azithromycin administered over five days. It is crucial to finish the full course once started to prevent the surviving bacteria from becoming even stronger.
Treatment duration varies significantly by age. Children under two generally need ten days of therapy. Those between two and five years with severe symptoms also require seven to ten days. Children over six with mild-to-moderate issues may manage with just five to seven days. Shortening the course too aggressively can lead to recurrence. Conversely, unnecessary long-term exposure contributes to gut microbiome disruption, often causing diarrhea in 10 to 25 percent of cases.
Managing Pain Before Medication Works
Pain control is the immediate priority regardless of antibiotic choice. Antibiotics take 24 to 48 hours to reduce infection load, leaving the child in pain for the first day of treatment. Administer acetaminophen or ibuprofen every four to six hours based on weight. Studies indicate that scheduled dosing manages discomfort far better than dosing only when crying begins. You can use ibuprofen (5 to 10 mg/kg/dose) or acetaminophen (10 to 15 mg/kg/dose).
Some parents consider ear drops, but caution is essential. Analgesic drops like Auralgan work well for topical relief. However, you should never use liquid drops if the eardrum has ruptured, as the solution enters the middle ear and could cause dizziness or hearing damage. Warm compresses applied to the outer ear can also soothe inflammation. If the child experiences severe pain unresponsive to analgesics, seek immediate care.
Prevention Strategies Beyond Vaccination
Vaccines play a massive role in reducing infection frequency. The PCV13 vaccine reduced vaccine-type pneumococcal AOM by 34 percent according to CDC surveillance data. More recently, the 15-valent pneumococcal conjugate vaccine (Vaxneuvance) approved in 2021 shows 85.1 percent efficacy against invasive disease. Beyond immunization, lifestyle factors matter immensely. Avoiding daycare reduces exposure by cutting down contact with sick peers, though this isn't always feasible for working families.
Eliminating secondhand smoke exposure is perhaps the most impactful environmental change. Smoke damages the cilia in the Eustachian tube that help clear mucus. Breastfeeding provides antibodies that support immune development and keeps the head upright during feeding, which aids drainage compared to bottle-feeding while lying horizontally. These steps collectively lower the incidence of future episodes.
Recognizing Complications and Red Flags
Most ear infections heal without permanent damage. However, chronic fluid can lead to conductive hearing loss of 15 to 40 decibels during active infection. If fluid persists for three months without clearing, hearing deficits may become significant. Monitor for red flags like facial weakness, severe dizziness, or pus draining from the ear, which indicates eardrum rupture. Recurrent cases, defined as three episodes in six months, warrant discussion with an ENT specialist. Procedures like myringotomy tubes can ventilate the middle ear to prevent further fluid buildup. Early identification of these issues prevents long-term developmental delays caused by temporary deafness.
How do I know if it is a virus or bacteria?
Doctors cannot tell instantly just by looking. Viral infections often accompany a runny nose and low-grade fever. Bacterial infections usually present with a red, bulging eardrum seen during otoscopy and higher fevers. If symptoms worsen after three days of home care, bacteria are likely involved.
Can I skip antibiotics for a mild infection?
Yes, for children over 24 months with mild symptoms, observation is recommended. You must monitor closely for worsening pain or fever spikes. If symptoms persist beyond 48 to 72 hours, medication is usually required then.
What if my child is allergic to Penicillin?
Options include Cefdinir, Azithromycin, or Ceftriaxone injections. Inform your doctor of the reaction history so they avoid cross-reactive medications safely.
Does breastfeeding actually prevent ear infections?
Yes, breastfeeding transfers protective antibodies. Additionally, the position during nursing helps keep the Eustachian tube open, whereas bottle-feeding lying down allows milk to enter the ear canal.
When should I call the doctor immediately?
Call immediately if the child has a fever over 104 degrees F, severe uncontrolled pain, dizziness, or fluid draining from the ear. These signs suggest rupture or serious complication requiring urgent assessment.


Julian Soro
April 1, 2026 AT 10:54The guidelines regarding amoxicillin dosing are spot on for preventing recurrence issues.
High dose protocols definitely help when dealing with resistant strains in younger kids.
We should remember that hydration supports immune function alongside the meds too.
Rocky Pabillore
April 2, 2026 AT 11:04Most parents simply cannot handle the waiting game suggested here.
They expect immediate solutions regardless of medical consensus.
It seems the modern population lacks the discipline required for watchful waiting protocols.
Jenny Gardner
April 3, 2026 AT 08:01The statistics on secondhand smoke are absolutely terrifying for child development!!!
How can anyone ignore a 50 percent increase in risk factors???
This information needs to be displayed in every pediatrician office immediately!!!!!
Arun Kumar
April 4, 2026 AT 04:03Caring for children with ear pain is a universal experience across different cultures.
In many parts of Asia we focus heavily on dietary changes during recovery periods.
Warm compresses are a remedy used globally before modern medicine arrived.
Sharon Munger
April 4, 2026 AT 18:26Prevention is better than cure.
I think avoiding smoke helps a lot too.
Christopher Beeson
April 6, 2026 AT 16:47Pain is the ultimate teacher of human fragility in the biological world.
We rush to suppress symptoms without honoring the body's struggle.
There is a certain nobility in suffering that modern medicine seeks to erase entirely.
Cara Duncan
April 8, 2026 AT 13:34While pain teaches us something, we should still ease it gently 😊
Managing discomfort helps the child sleep better 🌙
Balance is key in parenting decisions 💕
Eleanor Black
April 8, 2026 AT 18:19The structural nuances of the Eustachian tube in pediatric patients are often misunderstood by the layperson. Horizontal orientation creates a significant barrier for proper drainage mechanisms during respiratory illness. When we observe clinical outcomes across various demographics, the correlation between smoke exposure and infection rates becomes undeniable. It is crucial to recognize that fluid persistence does not always indicate active bacterial proliferation requiring immediate intervention. Many healthcare providers prioritize antibiotic administration due to liability concerns rather than evidence-based spontaneous resolution rates. This tendency undermines the efficacy of broader public health strategies aimed at reducing antimicrobial resistance over time. Parents frequently feel immense pressure to see tangible results before they can relax their vigilance regarding their child's well-being. Educational resources like this serve a vital function in bridging the gap between medical research and household application. Understanding the distinction between acute infection and effusion allows for more targeted symptom management instead of blind medication cycles. We must also acknowledge the psychological toll that recurrent ear infections place on family units during late night hours. Sleep disruption affects not only the child but the primary caregivers who manage the daily care routines. Implementing the watchful waiting protocol requires patience and trust in the body's natural healing processes which can be difficult to accept. Vaccination schedules represent another layer of defense that has significantly shifted the epidemiological landscape in recent decades. Continued investment in preventative care is essential to reduce the burden on emergency departments during peak flu seasons. Ultimately, informed decision-making empowers families to navigate these common pediatric challenges with greater confidence and less anxiety. :)
James DeZego
April 9, 2026 AT 14:30You mentioned the PCV13 vaccine stats earlier :-)
I work in a clinic and see fewer cases now with Vaxneuvance adoption.
It really helps reduce the invasive disease burden significantly!
Cullen Zelenka
April 10, 2026 AT 02:29This guide really covers the basics well for new parents.